
(Melanoma) Tumor Vaccine Information (Nature)
Medical Supporter — Information Notice
This article is a summary of international medical information and is not medical advice; it cannot replace the diagnosis or treatment plan of your attending physician. The medical technologies, drug information and clinical data presented here are compiled from public literature and official statements of major Japanese medical institutions; the applicability and outcome of any therapy vary with each patient and must be assessed individually by a qualified physician.
On July 5, those following developments in immune cell therapy would have seen exciting news in the journal Nature. Researchers from Dana-Farber Cancer Institute — the same institution associated with fusion cell therapy research — including Dr. Catherine Wu and colleagues at Germany's Universität Mainz, published results showing a breakthrough in Phase 1 clinical trials of a personalized cancer vaccine for melanoma.
This article also shares a publication on July 12 in Nature by Professor Cornelis J. M. Melief of Leiden University Medical Center (the Netherlands' oldest university), titled Precision T-Cell Therapy Targeting Tumours. The subtitle reads: The T cells of the immune system can destroy tumours, but their activation can be inefficient. Vaccines that exploit tumour mutations elicit robust T-cell responses to tumours, with potential clinical benefit.
In essence: while T cells of the immune system can destroy tumors, their activation efficiency is not always optimal. Vaccines can elicit robust T cell immune responses and offer potential clinical benefit.
As we have long been analyzing immune cell therapy advances, when people see "cancer vaccine," they often think of Kurume University's clinical trials using four peptide immunotherapy. Fusion cell therapy uses autologous cancer cells fused with dendritic cells, which are then infused back into the body to guide cytotoxic T cells (CTL) to attack cancer cells more precisely. There are many different production models for immune cell therapies; even when using the same type of cell, different approaches can lead to very different outcomes.
Here we introduce this study's approach and clinical results using the article's diagrams:
The trial target was melanoma. Anti-PD-1 antibody drugs (immune checkpoint inhibitors) are among the first-line treatments. The researchers used antigen-presenting cells (APCs) capable of carrying RNA to produce the vaccine.
a) CD4 and CD8 T cells attack if they recognize cancer cell surface antigens as foreign; if they recognize "self," they leave.
b) Once the cancer cell's PD-1 receptor is blocked, immune cells can attack.
c) With tumor vaccines, in Ott et al. and Sahin et al., Phase 1 clinical trials for skin cancer analyzed the antigen immune response. They analyzed antigens on the patients' tumors and manufactured personalized vaccines to activate or strengthen the immune response to these antigens. The authors observed tumor responses and immune responses; CD8+, CD4+ T cells responded to antigens in the vaccine.
d) Vaccination led to tumor destruction. Effective vaccines cause tumor shrinkage — but the article notes that in some patients, while tumors can be destroyed, cancer cell metastasis may occur, requiring PD-1 receptor blockade for complete destruction.
The trial involved melanoma patients who, after testing, received customized long-peptide vaccines comprising up to 20 synthesized neoantigens. From two clinical trials, some interesting figures emerged: among 13 published cases, follow-up at 8–12 months showed 8 patients with no detectable tumor, while 5 showed signs of recurrence. Of those 5, 1 had their tumor disappear after PD-1 treatment. Among the recurrent patients, 1 was found to have a mutation that eliminated MHC class I proteins, allowing tumor cells to evade immune mechanisms.
This article notes that Sahin and the research team pointed out: while the case numbers in this study are still small, the potential benefits of this therapeutic approach can be seen — for example, patients who received the vaccine and were followed up had a lower probability of recurrence and metastasis compared to their prior history. Additionally, if the tumor continues to grow, PD-1 receptor-targeted therapy can usually address this.
Current clinical results appear quite promising, but it should be noted that this remains a Phase 1 clinical trial with small sample sizes, and therefore broad interpretations should be avoided.
References:
- Personalized cancer vaccines show glimmers of success: https://www.nature.com/news/personalized-cancer-vaccines-show-glimmers-of-success-1.22249
- Precision T-cell therapy targets tumours: http://go.nature.com/2uNoHU5
- Antigen-presenting cell: https://en.wikipedia.org/wiki/Antigen-presenting_cell
Medical Supporter was formerly certified as an international medical visa guarantor by Japan's Ministry of Foreign Affairs and the Ministry of Economy, Trade and Industry (B-066).
Considering medical care in Japan? Need information and support?
We help you organize the information needed for medical travel to Japan, liaise with Japanese medical institutions, and arrange a second-opinion consultation.The first consultation is free; an advisor will help you clarify the next steps.
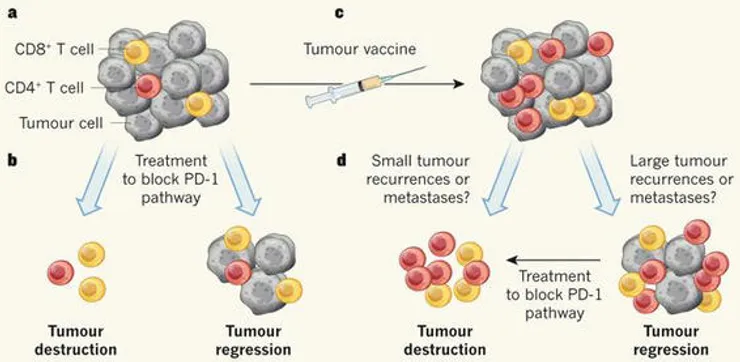 Figure 1
Figure 1
 Figure 2
Figure 2
 Figure 3
Figure 3
 Figure 4
Figure 4