
(Immunotherapy) Cancer Immunotherapy
Medical Supporter — Informationshinweis
Dieser Artikel ist eine Zusammenfassung internationaler medizinischer Informationen und stellt keine medizinische Beratung dar; er ersetzt nicht die Diagnose oder den Behandlungsplan Ihres behandelnden Arztes. Die dargestellten Informationen stammen aus öffentlichen Veröffentlichungen und offiziellen Angaben führender japanischer medizinischer Einrichtungen; Eignung und Wirkung einer Therapie sind individuell und müssen von einem qualifizierten Arzt beurteilt werden.
What is Immunity?
Immunity means the physiological system identifying self substances (self cells) versus foreign substances (non-self foreign matter), eliminating foreign matter. Cancer is healthy cell's uncontrolled growth from DNA damage producing malignant substances. The immune system recognizes cancerous cells as foreign.
Immune cells clearing cancer include natural (NK) cells, natural killer (NKT) cells, killer T cells (cytotoxic cells, also CTL). The most evolved is killer T cells. T cells differ from other immune cells in learning ability. Killer T cells' learning ability marks cancer cells, producing "cancer antigen" response, inducing powerful anti-cancer action.
What is Immunotherapy?
"Cancer immunotherapy" strengthens immune response treating cancer. Immune-related cells besides NK, NKT, killer T cells include macrophages, helper cells, B cells. Any method activating these cells achieving treatment goals qualifies as "cancer immunotherapy." It divides into antigen-nonspecific and specific. Cancer peptide vaccine therapy increasing killer T cells (activating them) preventing cancer recurrence or proliferation is specific immunotherapy.
Currently divides into cellular immunotherapy (immune cell therapy) and molecular immunotherapy (immune drug therapy). In Taiwan, molecular immunotherapy requires physician application approval; only cellular immunotherapy, limited by regulations not yet opened, requires other countries like China, Japan. Japan's cellular immunotherapy experience and medical technology level are high, making it the main choice for Taiwan patients.
Immunotherapy Classification
Immunotherapy divides into immune drug therapy and immune cell therapy.
Immune cells mainly derive from stem cell differentiation of leukocytes. 95% of leukocytes are granulocytes, 5% monocytes composing lymphocytes. Lymphocytes divide into B cells, T cells, NK cells, NKT cells. Currently widely-used immune cell therapies use NK cells, T cells, NKT cells, and dendritic cells.
Immune cell therapy broadly divides into two: nonspecific immune cell therapy activating immune cells without cancer cell characteristic recognition, and specific immune cell therapy allowing immune cell cancer cell recognition. Both involve NK, DC, T cells, or B cells.
Recent research showed αβT cells and γδT cells can be separated. Blood T lymphocytes are mostly αβT cells, containing several percent γδ receptor-proven. Previously T cells couldn't transmit antigen information, seemingly lacking cancer-cell attack ability, but γδT cells without dendritic cell instruction attack tumors like NK cells — this has been verified. Increasingly many institutions now practice this therapy.
Nonspecific Immune Cell Therapy
1. Cytokine Therapy
Cytokines are immune-related cell-released substances promoting immune cell activation and proliferation. Interleukin-2, interferon-alpha (IFN-α), interleukin-12, tumor necrosis factor (TNF) are administered via intravenous drip.
2. LAK = Lymphokine-Activated Killer Cells Therapy
This 1980s American therapy is the ancestor of various immune cell therapies. Mainly extracting large lymphocyte quantities from patient bodies then activating with interleukin-2, then reinjecting into patients. Mainly increasing NK cells, this does impose body burden on patients. Therefore CD3-LAK therapy will replace it.
3. NK = Natural Killer Cells Therapy
Extracting NK cells directly attacking cancer from patients, activating with interleukin-2, increasing quantity, then reinjecting into patients. Currently NK therapy compared to past shows multiplication from dozen-fold to thousand-fold increases. Currently many Japanese clinics practice this therapy, like the well-known Seta Clinic.
4. CAT = CD3-Activated T cells = CD3-LAK = αβT Cell Therapy
This therapy has many names, but identical content, and is currently the most prevalent. In cancer-attacking T cells, anti-CD3 antibodies (antibodies stimulating T cell CD3 molecules) and interleukin-2 are given, activating and proliferating therapy. Each cell ability compared to CTL not necessarily stronger, but can multiply in large quantities. These T cells mainly attack cancer cells; in αβ cell receptors CD8-positive T cells were discovered. These cells produce tumor-effective cytokine substances. This therapy's main body is cytotoxic T cells, also auxiliary activating T cells or NK cells. Many Japanese clinics practice this therapy; clinical experimental plans exist, like Tokyo Women's Medical University Medical Center.
5. Allogeneic Lymphocyte Therapy
This therapy uses other people's lymphocytes injected into patients, stimulating patients' self lymphocytes increasing lethality. However this does not involve injecting cancer-attacking lymphocytes; it mainly relies on the patient's own immune system. This therapy originated from 1972 Harvard University mouse experiments. Same strain mice lymphocyte injection proved effective, then other animal trials progressed to human clinical trials. Results proved other people's lymphocyte injection increased patient self lymphocytes' cancer-cell attack effects.
This therapy uses NK cells and dendritic cells first enabling cancer cell recognition then attacking — a nonspecific immunotherapy type. Individually, cancer-killing force is greater than T cells. The advantage of this therapy uses other people's lymphocytes, therefore not requiring patient blood extraction. Single injection 20cc–40cc, burden is not excessive. Note: since injecting other people's lymphocytes, watch for virus infection.
Specific Immune Cell Therapy
1. CTL = Cytotoxic T Lymphocytes Therapy
Extracting cancer-attacking T cells from patients, making them recognize patient's own cancer cells or cancer antigen proteins. T cells learn cancer-cell recognition, interleukin-2 cultivating, activating anti-CD3 antibodies, producing large cytotoxic T lymphocytes, then reinjecting into patients.
CTL therapy has T-CTL from patient's antigen extraction and P-CTL artificial antigen types. Compared to self-cancer antigens, P-CTL is deemed more effective. T-CTL therapy is limited to surgical method extracting larger tumor antigens. P-CTL therapy must recognize cancer cells through MHC molecule antigens. This is CTL therapy's main disadvantage.
2. TIL = Tumor Infiltrating Lymphocytes Therapy
Lymphocytes extracted from tumors possess cancer antigen, collecting activated T cells. From tumor collection using interleukin-2 cultivation, then reinjecting into patients. However tumor tissue lymphocyte separation methods are troublesome; after long cultivation and reinjection, tumor benefits await enhancement. Currently a new method tries TIL cells and cancer cells co-cultivation, enabling stronger tumor effects, currently under discussion.
3. DC = Dendritic Cell Therapy
DC is one antigen-presenting cell, effective at stimulating and activating T cells to become killer T cells, attacking cancer cells. One DC stimulates hundreds to thousands of lymphocytes, quite efficient. However DC quantity only occupies 0.1–0.5% of white blood cells. Currently used DC therapy extracts more immune cells than DC monocytes from blood achieving component separation to obtain large quantities, then drug-differentiated to produce DC using new technology.
DC therapy currently uses patient tumor antigens or artificial antigens mixing, enabling DC to more easily activate T cells, then reinjecting DC vaccine therapy into patients. For non-surgical patients, DC1 therapy is also possible.
This DC therapy, enabling DC better antigen-presentation, developed CHP complex vaccines. This is a pullulan-sugar-wrapped HER2 cancer antigen protein synthesis vaccine. In animal experiments, after CHP vaccine injection, DC antigen-presenting cells' cancer antigen presentation efficiency increases, and NKT cancer-cell attack benefits markedly increase. Currently this clinical experiment proceeds at Japan's Mie University, mainly targeting breast cancer, esophageal cancer, and lung cancer.
4. Neoantigen = Novel Antigen
Also using dendritic cells, but with a different antigen-presentation method. This method requires patient living tumor tissue cell gene testing, confirming cancer cell surface antigens, then tailor-made education of dendritic cells, enabling T cells to receive more tumor information, achieving cancer-cell attack goals. In July 2017 and June 2018, world-famous biotech magazines Science and Nature Medicine mentioned related clinical data, notably combining immune checkpoint inhibitors.
Nonspecific and Specific Combined Immune Cell Therapy
1. CTL + NKT Therapy
This newest proven NKT cell application therapy. Past therapies used CTL enabling T cells cancer-cell recognition then reinject body treatment. But this only targets cancer MHC antigen molecules; if cancer cells lose MHC antigen molecules, they go unrecognized. Therefore NKT cells are used to attack MHC antigen-losing cancer cells. NKT cells and NK cells have identical function — DC cells receiving cancer cell antigen presentation immediately attack cancer cells. Therefore one therapy uses two immune cell types complementing each other. Currently anticipated, Chiba University Medical Department performs clinical experiments.
2. γδT Cell Therapy / BAK Therapy (BRM Activated Killer)
γδT cells in lymphocytes occupy only several percent. These cells without DC instruction actively attack cancer cells. Additionally γδT cells possess anti-tumor effects, producing INTγ and other cytokines, but they gradually decline with age. This therapy was developed by Dr. Takushiro Ebina at Miyagi Cancer Center Research Institute. From patients extracting γδT cells from blood NK cells' CD56-positive lymphocytes, after two-week cultivation, they are reinjected into patients. Clinical effects show two complete relief cases, one partial relief case, and ten continuous stability cases. For post-surgery metastasis prevention using BAK therapy in four patients, two showed no relapse signs.
For any immune cell therapy questions, please contact us through the methods below.
Medical Supporter was formerly certified as an international medical visa guarantor by Japan's Ministry of Foreign Affairs and the Ministry of Economy, Trade and Industry (B-066).
Behandlung in Japan im Blick? Brauchen Sie Informationen und Unterstützung?
Wir helfen Ihnen, die für eine medizinische Reise nach Japan nötigen Informationen zu ordnen, kontaktieren japanische Einrichtungen und organisieren eine Zweitmeinungsberatung.Die Erstberatung ist kostenlos; ein Berater hilft Ihnen, die nächsten Schritte zu klären.
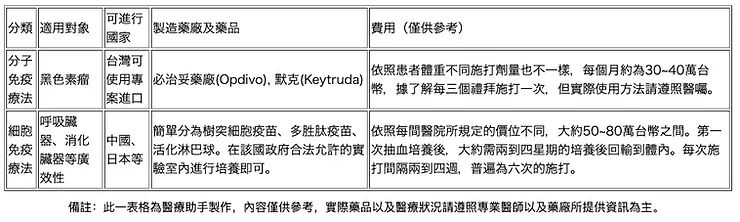 Figure 1
Figure 1
 Figure 2
Figure 2
 Figure 3
Figure 3
 Figure 4
Figure 4
 Figure 5
Figure 5